

Essential Facts and Figures – COVID-19
Italian COVID-19 patients are isolated in a makeshift hospital to prevent them causing outbreaks in ordinary hospitals.
This page aims to summarise our understanding of the current science on key questions about COVID-19 (as of 3 April, 2020), as best we can given the state of the evidence and the fast moving situation. We provide more explanation as well as sources in the footnotes.
Table of Contents
Symptoms and severity
- The most common reported symptoms are cough (appearing in about 80% of confirmed cases – meaning those who have been tested and found to be infected with the virus) and fever (80%-90%).%22Clinical Characteristics of Coronavirus Disease 2019 in China"</a> found fever in 43.8% of patients upon admission to a hospital and 88.7% during hospitalization. A 30 January paper <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401122419/https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30211-7/fulltext">"Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study"</a> found that upon admission to the hospital, 83% of patients had a fever, 82% had a cough, and 31% had shortness of breath. The <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html">CDC lists</a> fever, cough, and shortness of breath as symptoms to watch for.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">1 Many also experience shortness of breath, usually later in the disease progression. Diarrhea and other GI symptoms have also been seen in some patients.here, 84% of COVID-19 patients experienced loss of appetite, 29% had diarrhea, 0.8% experienced vomiting, and 0.4% had abdominal pain. It's hard to draw a conclusion here, because some of this contradicts earlier evidence from <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401122649/https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30211-7/fulltext">the 28 February paper</a> cited in the previous footnote, which found diarrhea in only 2% of cases at admission.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">2 Nasal congestion and runny nose seem uncommon (<5%).The 30 January paper from footnote 1 </a> found sore throat at admission in 5% of patients and runny nose (rhinorrhoea) in 4%.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">3 Anecdotally, loss of the sense of taste or smell have also been reported.See for instance this New York Times article from 22 March</a></p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">4
- Once someone is infected, it seems to typically take ~7 days for symptoms to develop. One study with a large sample size found that for 11.5% of confirmed cases it took more than 14 days. "Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia"</a> and a 10 March paper, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123026/https://annals.org/aim/fullarticle/2762808/incubation-period-coronavirus-disease-2019-covid-19-from-publicly-reported">"The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application"</a> found a mean and median (respectively) incubation period of around 5 days. <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200402-sitrep-73-covid-19.pdf?sfvrsn=5ae25bc7_2%22>The World Health Organization reports similar figures.</a> However, a 18 March preprint <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.medrxiv.org/content/10.1101/2020.03.15.20036533v1">"Is a 14-day quarantine period optimal for effectively controlling coronavirus disease 2019 (COVID-19)?"</a> suggests longer incubation periods. Based on a wider range of cases (2015 compared to 181 for the March 10 paper and 425 for the March 26 paper), the authors found incubation periods ranging from 0 to 33 days with a median of 7 days. It's not fully clear to me what accounts for the difference here, since all the above studies were based on confirmed cases, in China, in January and February. However, the last study's large sample size and explicit attempt to include less severe cases make its finding seem more reliable. The authors of that study also report longer incubation periods for children and people who seem to have been infected via food rather than breathing in droplets (both with a median of 9 days).</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">5
- According to initial data from China, around 81% of confirmed cases are ‘mild’ (though can still involve pneumonia), 14% are severe (requiring hospitalisation), and 5% are critical.The Chinese CDC</a> found that 80.9% of cases reported in China up to 11 February were 'mild', meaning without pneumonia or with only mild pneumonia (so you can still feel quite sick with a mild case), 13.8% were 'severe', involving shortness of breath and lower blood oxygen levels, and 4.7% were 'critical', meaning they had respiratory failure, septic shock or organ failure. See Table 1 for the figures and 'Variables' for the definitions.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">6 A large proportion of people infected with the virus have mild symptoms, and around 20% may have no symptoms,As reported by the Centers for Disease Control</a>, testing on the Diamond Princess cruise ship found 46.5% of passengers who tested positive were asymptomatic at the time of testing. However, COVID-19 has a long incubation period, and these people may have become symptomatic later. <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123207/https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e3.htm?s_cid=mm6912e3_w%22>A 26 March follow up</a> suggested based on modeling that 17.9% of those who tested positive never developed symptoms.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">7 though there is not reliable data here.
- Most current estimates of the fraction of infected people (rather than people with confirmed cases) who die from the disease (the ‘IFR’) seem to be between 0.1% and 2%."Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand"</a> uses a 0.9% (95% credible interval 0.4%-1.4%) infection fatality rate for the UK in its analysis. Their estimate comes from making adjustments to the 13 March preprint <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200324094225/https://www.medrxiv.org/content/10.1101/2020.03.09.20033357v1">"Estimates of the severity of COVID-19 disease"</a>, which finds a 0.66% infection fatality rate for China with a 95% credible interval of 0.39% to 1.33%. A 6 March preprint, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200324094618/https://www.medrxiv.org/content/10.1101/2020.03.04.20031104v1">"Adjusted age-specific case fatality ratio during the COVID-19 epidemic in Hubei, China, January and February 2020"</a>, found a rate of 1.6% (1.4%-1.8%). The report <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123312/https://institutefordiseasemodeling.github.io/nCoV-public/analyses/first_adjusted_mortality_estimates_and_risk_assessment/2019-nCoV-preliminary_age_and_time_adjusted_mortality_rates_and_pandemic_risk_assessment.html">"2019-nCoV: preliminary estimates of the confirmed-case-fatality-ratio and infection-fatality-ratio, and initial pandemic risk assessment"</a> (updated 19 February) found an infection fatality rate for China of 0.94% (0.37% to 2.9%). <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.cebm.net/covid-19/global-covid-19-case-fatality-rates/">A very recent (29 March) estimate from Oxford's Center for Evidence Based Medicine</a> puts the worldwide infection fatality rate considerably lower: "Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR between 0.1% and 0.26%."</p> <p>Even if the worldwide IFR is relatively low right now, it would not be surprising if infection fatality rates were considerably higher in places where the medical system is overwhelmed, such as Italy, or in the future if the infection spreads to a greater proportion of the population and hospitals are overwhelmed in more places.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">8 The fraction will vary based on whether healthcare capacity is overwhelmed, as well as the age and health of the population. One reason estimates are uncertain is that we don’t know how many mild and symptom-free cases there are, which usually go unconfirmed; if there are more, the IFR is lower.
- Risks of long-term health effects are unknown because not enough time has passed, though there are concerns that some portion of COVID-19 patients (perhaps those with more severe cases) might face ongoing issues like reduced lung capacity.There have been some early reports of reduced lung function after recovery from COVID-19</a>, but no strong evidence. Speculation based on other diseases is inconclusive. COVID-19 is more severe than the common cold and less severe than SARS1 from 2003. The common cold doesn't result in long-term effects, but <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123751/https://www.ncbi.nlm.nih.gov/pubmed/20008700">according to one study</a> some survivors of SARS1 reported suffering from ongoing lung problems or chronic fatigue.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">9
Who is most at risk?
- Children can catch and spread the virus, though they may be less likely to, and they rarely have serious symptoms."16-24 February Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)"</a> found that "Within Wuhan, among testing of ILI samples, no children were positive in November and December of 2019 and in the first two weeks of January 2020." However, that report also emphasizes that we cannot draw conclusions from the data available -- perhaps because children were less likely to be tested at all. And a 27 March preprint <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123414/https://www.medrxiv.org/content/10.1101/2020.03.03.20028423v3">"Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts"</a> suggests children are at a similar risk of infecting others as adults. We haven't had time to look into this topic. What does seem clear is that children are in much less danger themselves. But it seems likely that mild and asymptomatic cases can still be infectious (see footnote 15), so even then children can likely still infect others.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">10
- Men seem to be about 50% more likely to die of the disease than women on average.joint mission report</a> cited above reports a case fatality rate for the studied patients higher among men vs. women (4.7% vs. 2.8%), and a <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401123503/http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51">21 February report from the Chinese CDC</a> found a case fatality rate for men of 2.8% v.s. 1.7% for women. It's not clear, however, whether this difference is attributable to sex or something else that correlates with sex.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">11
- Age is a large risk factor for mortality, as suggested in the set of estimates in the table below, used by researchers at Imperial College London. The estimates are for infections (rather than for confirmed cases) and based on data from the early phase of the disease in China:
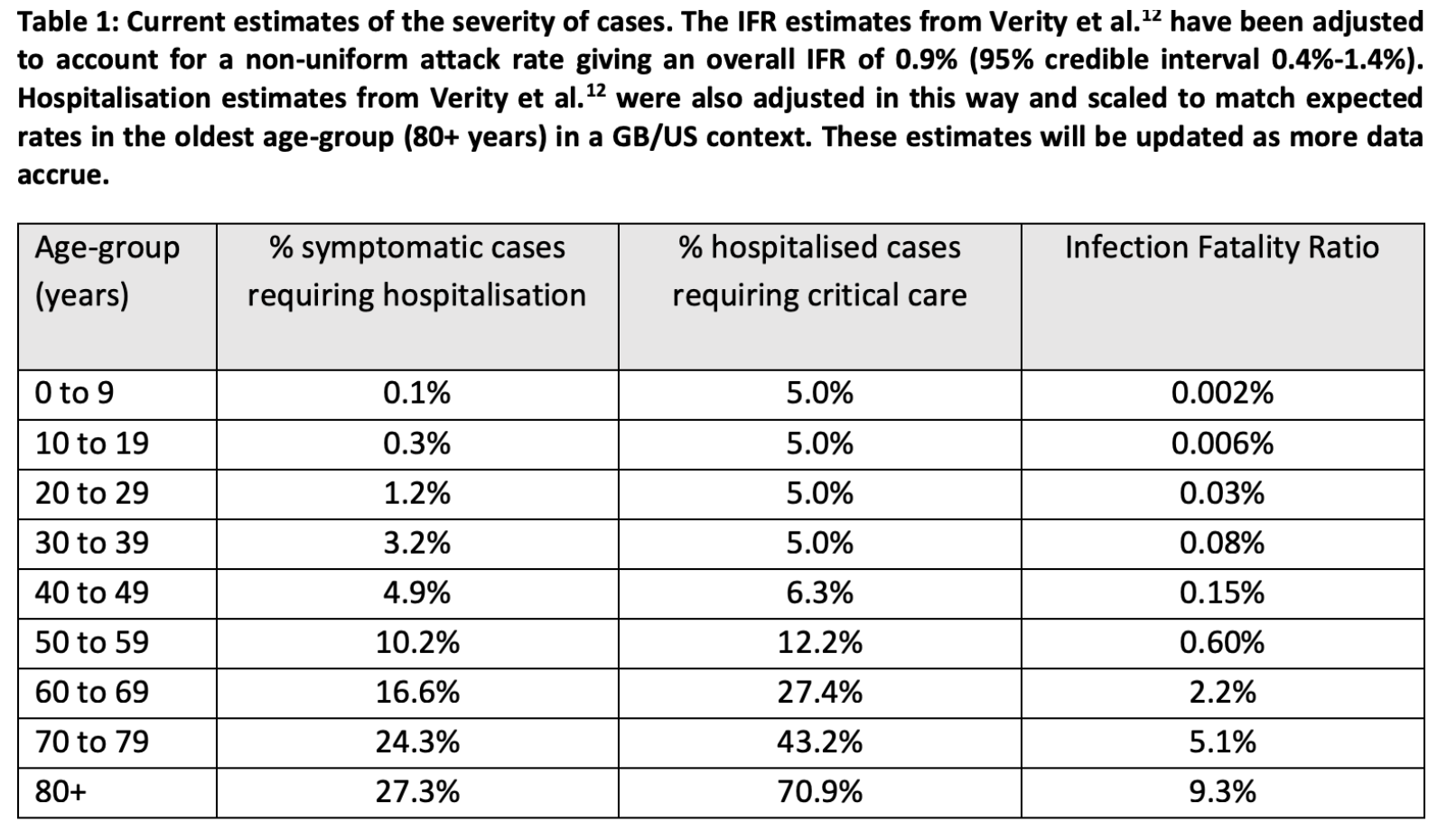
Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand
How is the virus spread?
- How COVID-19 spreads is not fully understood, but most experts seem to think droplets from coughs and sneezes are most important. ‘Aerosols’ — smaller droplets that can be expelled even while talking and hang in the air longer — may also be significant.The Center for Disease Control</a> and <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.who.int/news-room/q-a-detail/q-a-coronaviruses">the World Health Organization</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">12
- This means the main ways you can become infected are by being close to someone talking, coughing, or sneezing, and by touching an infected surface and then touching your face. Sources commonly recommend staying six feet away from others, but this just is a best guess for how far viral particles can travel through the air, and further is of course safer. On plastic and stainless steel, virus particles can remain viable for three days or more; they remain viable for less time on copper and cardboard."Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1"</a>, found that the novel coronavirus survives for a shorter time on copper and cardboard, and longer on stainless steel and plastic. The results for cardboard are more uncertain than for the other surfaces.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">13
- It’s thought that people can be infectious perhaps one or two days before they develop symptoms, though they’re less infectious than when they have symptoms."Temporal dynamics in viral shedding and transmissibility of COVID-19"</a> estimates that infectiousness peaks on or before the onset of symptoms, based on finding the highest amount of virus in patients' throats at the time of symptom onset. They further suggested that a substantial amount of transmission could occur before the onset of symptoms. <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401124030/https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf">The Imperial College London paper</a> cited above assumed that transmission was possible 12 hours before the onset of symptoms. Suggestively, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.nhs.uk/common-health-questions/infections/how-long-is-someone-infectious-after-a-viral-infection/">the common cold is transmissible up to a few days before symptoms begin</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">14 Totally asymptomatic people (including children) may also be infectious. It’s currently debated how much transmission is driven by asymptomatic and very mild cases."Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus"(SARS-CoV2)"</a> tried to find how much of COVID-19's spread was due to these unrecognized cases in China, and reported that "Per person, the transmission rate of undocumented infections was 55% of documented infections ([46%–62%])." However, we don't know how mild the symptoms were in these undocumented infections. In general, there is controversy about the relationship between symptoms and infectiousness.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">15
- It’s unknown how long people stay infectious after they develop symptoms. The CDC recommends home isolation for seven days after symptoms start and three days after they resolve. By contrast, the WHO recommends isolation for 14 days after symptoms resolve.16
How many will be infected?
- You can track the total number of confirmed cases and deaths attributed to COVID-19 by country on the Johns Hopkins dashboard (or see here if you want a lot more detail).
- The number of infections is higher than the number of confirmed cases everywhere. By how much depends on how extensive testing is, which varies extremely widely – it seems plausible some countries could be capturing up to half of infections while others are capturing as little as 1% (or even less).data collected by Our World in Data</a>, by 14 March the US (population 327 million) had done 37,646 tests; Japan (127 million) had done 14,901 by 19 March, and India (1.3 billion) had done 14,514 by 20 March. On the other hand, by 20 March South Korea (51 million) had done 316,664 tests and Taiwan (24 million) had done 21,376. This suggests large variation in the number of cases being captured in each country.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">17
- How many will eventually become infected (and how quickly) depends on how we respond. If spread is uncontrolled, models suggest that at the start of the epidemic each infected person will infect on average another ~2-6 people (and perhaps more).Imperial College London paper cited above</a> assumes that each person will on average infect 2.4 people, based on early transmission data from Wuhan. A newer (30 March) paper from Imperial, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-Europe-estimates-and-NPI-impact-30-03-2020.pdf">"Estimating the number of infections and the impact of nonpharmaceutical interventions on COVID-19 in 11 European countries"</a> estimates that without interventions in Europe the average R0 across 11 countries was 3.57 (95% credible interval 3.01-4.66). A 7 April "early release" paper published on the CDC's website, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article">"High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2"</a> found a much higher R0 of 5.7 for early transmission in China, with a credible interval of between 3.8 and a shockingly high 8.9. The 30 March paper from Imperial found that interventions implemented in the studied countries caused a reduction of 64% in the R0 on average.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">18 Interventions like social distancing reduce this number substantially. If each person infects between 2 and 6 others, it’s been estimated that ~50-80% of the population would need to develop immunity (most likely through being infected and surviving) in order for the population as a whole to have “herd immunity.”the 7 April "early release" cited in the previous footnote</a>, according to which for an R0 of 2.2 the threshold for herd immunity is 55%, and for and R0 of 5.7 it is 82%" The threshold for herd immunity could be even higher if, as the authors of that paper say might have been the case in the early days of the epidemic in Wuhan, the R0 is even higher than 5.7. The UK's chief scientific advisor Patrick Vallance gave a figure of 60% for the UK in mid-march, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/web/20200401124235/https://news.sky.com/story/coronavirus-millions-of-britons-will-need-to-contract-covid-19-for-herd-immunity-11956793">as reported by Sky News</a> and repeated in the <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.ft.com/content/38a81588-6508-11ea-b3f3-fe4680ea68b5">Financial Times</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">19. If the virus spreads uncontrolled worldwide, this would likely result in tens of millions of deaths.
- However, many governments are now acting to suppress the spread. The best all-things-considered forecasts we know for total eventual reported cases and mortality are from the Good Judgement Project. For example, as of 3 April, forecasters think there’s a 24% chance that more than 8 million people will die worldwide from COVID-19 before 31 March, 2021 and a 17% chance that less than 800,000 will.
Reducing the risk of infection
- The most highly recommended ways of limiting the spread are staying home, limiting contact with others, washing hands thoroughly, and covering coughs and sneezes with a tissue.NHS, the <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html">CDC, and the <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.coronavirus.gov.hk/eng/health-advice.html">Hong Kong government</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">20 If you want to go all out see the guidelines for individuals from endcoronavirus.org.
- Getting plenty of sleep and exercise can help strengthen your immune system.here. It's worth noting that in <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.sciencemag.org/news/2020/03/not-wearing-masks-protect-against-coronavirus-big-mistake-top-chinese-scientist-says">an interview with the American Association for the Advancement of Science</a> George Gao, director-general of the Chinese Center for Disease Control and Prevention, says he thinks not using masks to help control the pandemic in the West is a mistake.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">21 We’ve also heard some evidence that Vitamin D reduces the frequency or severity of respiratory infections, though this is a less common recommendation.
- Expert consensus seems to be that wearing a surgical mask does help prevent you from infecting others. Due to the shortage among healthcare workers, healthy members of the public shouldn’t buy surgical masks (or N-95s) at the moment. For this reason, we opted not to review the evidence for apparently healthy people wearing surgical masks in ordinary life, though our impression is that they do offer some measure of protection.here. It's worth noting that in <a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.sciencemag.org/news/2020/03/not-wearing-masks-protect-against-coronavirus-big-mistake-top-chinese-scientist-says">an interview with the American Association for the Advancement of Science</a> George Gao, director-general of the Chinese Center for Disease Control and Prevention, says he thinks not using masks to help control the pandemic in the West is a mistake.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">21
- Homemade masks have not been rigorously tested, so we have to rely on weaker forms of evidence. The jury is still out on whether homemade masks are overall helpful, but there’s a common-sense case in their favour, and their use in some circumstances has recently been endorsed by the US CDC.This post</a> makes the case for using homemade masks to help decrease transmission.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">22
Treatments
- There is currently no vaccine or other proven pharmaceuticals. The main treatments provided by hospitals are things like life support in severe cases (e.g. assistance breathing) so patients live long enough for their immune systems to eliminate the virus.
- Blood plasma from recovered COVID-19 patients has been used with some success in treating critically ill cases. The treatment has not been thoroughly tested or approved, but results from early cases of “compassionate use” seem promising.the FDA announced plans to develop blood therapies, including convalescent plasma, for COVID-19</a>, while allowing their simultaneous use for critically ill cases without other options. The sense of promise for these therapies is based on past successes treating other respiratory viruses with these methods as well as preliminary reports of improvement in COVID-19 patients given plasma (<a href=https://80000hours.org/articles/covid-19-key-facts/"https://www.medrxiv.org/content/10.1101/2020.03.16.20036145v1">1, <a href=https://80000hours.org/articles/covid-19-key-facts/"https://jamanetwork.com/journals/jama/fullarticle/2763983">2). These reports are not from controlled trials, which have not been conducted, and are based on use in 10 and 5 cases, respectively.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">23 Unfortunately, scaling up this treatment is a challenge because it requires blood from donors.
- There are many trials of antivirals being undertaken, which could reduce severity. It’s very hard to predict, but it seems plausible we could see some antivirals developed within a year.This 22 March article from the American Association for the Advancement of Science</a> gives a helpful overview of different treatments being trialed and what we know about timelines for development. <a href=https://80000hours.org/articles/covid-19-key-facts/"https://web.archive.org/save/https://www.statnews.com/2020/03/24/when-might-experimental-drugs-to-treat-covid-19-be-ready-a-forecast/">Here is another, similar article in STAT from 24 March</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">24
- Developing a vaccine will take at least a year, and potentially several years.One such article from The Guardian (updated on 1 April) is here</a>.</p> " rel="footnote" class="footnote-link no-visited-styling" aria-label="Footnote">25
Learn more: we made a list of other primers on COVID-19.
How can you help the world tackle COVID-19?
It’s still possible to greatly reduce the damage and death caused by COVID-19. See our guide for helping tackle the crisis, and for donating to work on COVID-19, as well as all our other advice and analysis about COVID-19.
Notes and references
- A great deal of research has been published on COVID-19 symptoms. Our figures are based on the following (which as far as we can tell are roughly in line with most other studies): a 28 February paper, “Clinical Characteristics of Coronavirus Disease 2019 in China” found fever in 43.8% of patients upon admission to a hospital and 88.7% during hospitalization. A 30 January paper “Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study” found that upon admission to the hospital, 83% of patients had a fever, 82% had a cough, and 31% had shortness of breath. The CDC lists fever, cough, and shortness of breath as symptoms to watch for.↩
- According to investigators from the Wuhan Medical Treatment Expert Group for COVID-19 as reported here, 84% of COVID-19 patients experienced loss of appetite, 29% had diarrhea, 0.8% experienced vomiting, and 0.4% had abdominal pain. It’s hard to draw a conclusion here, because some of this contradicts earlier evidence from the 28 February paper cited in the previous footnote, which found diarrhea in only 2% of cases at admission.↩
- The 30 January paper from footnote 1 found sore throat at admission in 5% of patients and runny nose (rhinorrhoea) in 4%.↩
- See for instance this New York Times article from 22 March↩
- A 26 March paper “Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia” and a 10 March paper, “The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application” found a mean and median (respectively) incubation period of around 5 days. The World Health Organization reports similar figures. However, a 18 March preprint “Is a 14-day quarantine period optimal for effectively controlling coronavirus disease 2019 (COVID-19)?” suggests longer incubation periods. Based on a wider range of cases (2015 compared to 181 for the March 10 paper and 425 for the March 26 paper), the authors found incubation periods ranging from 0 to 33 days with a median of 7 days. It’s not fully clear to me what accounts for the difference here, since all the above studies were based on confirmed cases, in China, in January and February. However, the last study’s large sample size and explicit attempt to include less severe cases make its finding seem more reliable. The authors of that study also report longer incubation periods for children and people who seem to have been infected via food rather than breathing in droplets (both with a median of 9 days).↩
- The Chinese CDC found that 80.9% of cases reported in China up to 11 February were ‘mild’, meaning without pneumonia or with only mild pneumonia (so you can still feel quite sick with a mild case), 13.8% were ‘severe’, involving shortness of breath and lower blood oxygen levels, and 4.7% were ‘critical’, meaning they had respiratory failure, septic shock or organ failure. See Table 1 for the figures and ‘Variables’ for the definitions.↩
- As reported by the Centers for Disease Control, testing on the Diamond Princess cruise ship found 46.5% of passengers who tested positive were asymptomatic at the time of testing. However, COVID-19 has a long incubation period, and these people may have become symptomatic later. A 26 March follow up suggested based on modeling that 17.9% of those who tested positive never developed symptoms.↩
- The influential 6 March paper “Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand” uses a 0.9% (95% credible interval 0.4%-1.4%) infection fatality rate for the UK in its analysis. Their estimate comes from making adjustments to the 13 March preprint “Estimates of the severity of COVID-19 disease”, which finds a 0.66% infection fatality rate for China with a 95% credible interval of 0.39% to 1.33%. A 6 March preprint, “Adjusted age-specific case fatality ratio during the COVID-19 epidemic in Hubei, China, January and February 2020”, found a rate of 1.6% (1.4%-1.8%). The report “2019-nCoV: preliminary estimates of the confirmed-case-fatality-ratio and infection-fatality-ratio, and initial pandemic risk assessment” (updated 19 February) found an infection fatality rate for China of 0.94% (0.37% to 2.9%). A very recent (29 March) estimate from Oxford’s Center for Evidence Based Medicine puts the worldwide infection fatality rate considerably lower: “Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR between 0.1% and 0.26%.”
Even if the worldwide IFR is relatively low right now, it would not be surprising if infection fatality rates were considerably higher in places where the medical system is overwhelmed, such as Italy, or in the future if the infection spreads to a greater proportion of the population and hospitals are overwhelmed in more places.↩
- There have been some early reports of reduced lung function after recovery from COVID-19, but no strong evidence. Speculation based on other diseases is inconclusive. COVID-19 is more severe than the common cold and less severe than SARS1 from 2003. The common cold doesn’t result in long-term effects, but according to one study some survivors of SARS1 reported suffering from ongoing lung problems or chronic fatigue.↩
- Some studies seem to indicate that children are not only less likely to be symptomatic, they are less likely to catch the virus. For instance, the “16-24 February Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)” found that “Within Wuhan, among testing of ILI samples, no children were positive in November and December of 2019 and in the first two weeks of January 2020.” However, that report also emphasizes that we cannot draw conclusions from the data available — perhaps because children were less likely to be tested at all. And a 27 March preprint “Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts” suggests children are at a similar risk of infecting others as adults. We haven’t had time to look into this topic. What does seem clear is that children are in much less danger themselves. But it seems likely that mild and asymptomatic cases can still be infectious (see footnote 15), so even then children can likely still infect others.↩
- The joint mission report cited above reports a case fatality rate for the studied patients higher among men vs. women (4.7% vs. 2.8%), and a 21 February report from the Chinese CDC found a case fatality rate for men of 2.8% v.s. 1.7% for women. It’s not clear, however, whether this difference is attributable to sex or something else that correlates with sex.↩
- See guidelines from The Center for Disease Control and the World Health Organization.↩
- A 17 March “correspondence,” in the New England Journal of Medicine, “Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1”, found that the novel coronavirus survives for a shorter time on copper and cardboard, and longer on stainless steel and plastic. The results for cardboard are more uncertain than for the other surfaces.↩
- It seems very likely there is at least some infectious period before symptoms develop. An 18 March preprint “Temporal dynamics in viral shedding and transmissibility of COVID-19” estimates that infectiousness peaks on or before the onset of symptoms, based on finding the highest amount of virus in patients’ throats at the time of symptom onset. They further suggested that a substantial amount of transmission could occur before the onset of symptoms. The Imperial College London paper cited above assumed that transmission was possible 12 hours before the onset of symptoms. Suggestively, the common cold is transmissible up to a few days before symptoms begin.↩
- It’s difficult to know how much transmission is due to mild and asymptomatic cases, as they usually go unrecognized. A 16 March paper “Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus”(SARS-CoV2)” tried to find how much of COVID-19’s spread was due to these unrecognized cases in China, and reported that “Per person, the transmission rate of undocumented infections was 55% of documented infections ([46%–62%]).” However, we don’t know how mild the symptoms were in these undocumented infections. In general, there is controversy about the relationship between symptoms and infectiousness.↩
- Up To Date’s guidelines on home care cite the CDC and WHO recommendations. There is some reason to think infectiousness peaks at the beginning of symptoms (see footnote 14), though even if that’s right we don’t know how long it takes to subside after that.↩
- According to data collected by Our World in Data, by 14 March the US (population 327 million) had done 37,646 tests; Japan (127 million) had done 14,901 by 19 March, and India (1.3 billion) had done 14,514 by 20 March. On the other hand, by 20 March South Korea (51 million) had done 316,664 tests and Taiwan (24 million) had done 21,376. This suggests large variation in the number of cases being captured in each country.↩
- The average number of people each infected person infects (the ‘R0’), is uncertain and changes with circumstance. The Imperial College London paper cited above assumes that each person will on average infect 2.4 people, based on early transmission data from Wuhan. A newer (30 March) paper from Imperial, “Estimating the number of infections and the impact of nonpharmaceutical interventions on COVID-19 in 11 European countries” estimates that without interventions in Europe the average R0 across 11 countries was 3.57 (95% credible interval 3.01-4.66). A 7 April “early release” paper published on the CDC’s website, “High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2” found a much higher R0 of 5.7 for early transmission in China, with a credible interval of between 3.8 and a shockingly high 8.9. The 30 March paper from Imperial found that interventions implemented in the studied countries caused a reduction of 64% in the R0 on average.↩
- “Herd immunity” is a phenomenon whereby a large enough portion of a population is immune to a virus, whether because they have already been infected or from vaccination, that the virus is mostly unable to spread in the population, even to those not immune. The threshold of infection for a population to have herd immunity depends on how many people the average infected person infects (the ‘R0’), and how common and long lasting immunity is (which is unknown for those who have been infected with COVID-19, but thought to be reasonably common and long-lasting, as with other coronaviruses), among other things. The 50-80% figure comes from the 7 April “early release” cited in the previous footnote, according to which for an R0 of 2.2 the threshold for herd immunity is 55%, and for and R0 of 5.7 it is 82%” The threshold for herd immunity could be even higher if, as the authors of that paper say might have been the case in the early days of the epidemic in Wuhan, the R0 is even higher than 5.7. The UK’s chief scientific advisor Patrick Vallance gave a figure of 60% for the UK in mid-march, as reported by Sky News and repeated in the Financial Times.↩
- This is the main advice we’ve seen from many sources — though different institutions have slightly different recommendations. See e.g., guidelines from the NHS, the CDC, and the Hong Kong government.↩
- You can see a review of the evidence that surgical masks reduce infection for the mask wearer here. It’s worth noting that in an interview with the American Association for the Advancement of Science George Gao, director-general of the Chinese Center for Disease Control and Prevention, says he thinks not using masks to help control the pandemic in the West is a mistake.↩
- Some worry that homemade face masks could cause or worsen infections by capturing viruses and bringing them closer to the face, or if they are shared or not washed. They might also give people a false sense of security, causing people to be more cavalier about going out and being near other people, and even proponents agree they are not highly effective at preventing infection, either for the wearer or those around them. All that said, they may be better than nothing. This post makes the case for using homemade masks to help decrease transmission.↩
- On 3 April the FDA announced plans to develop blood therapies, including convalescent plasma, for COVID-19, while allowing their simultaneous use for critically ill cases without other options. The sense of promise for these therapies is based on past successes treating other respiratory viruses with these methods as well as preliminary reports of improvement in COVID-19 patients given plasma (1, 2). These reports are not from controlled trials, which have not been conducted, and are based on use in 10 and 5 cases, respectively.↩
- This 22 March article from the American Association for the Advancement of Science gives a helpful overview of different treatments being trialed and what we know about timelines for development. Here is another, similar article in STAT from 24 March.↩
- We did not draw this estimate from a single source, but rather from a variety of popular articles discussing the necessary steps and typical obstacles in vaccine development. One such article from The Guardian (updated on 1 April) is here.↩